

Denmark has Europe's highest cancer incidence
- jearungby
- Dec 25, 2025
- 12 min read
By Jeanne A. Rungby, MD, specialist.
On December 19, Jesper Fisker, CEO of the Danish Cancer Society, writes in Sundhedspolitisk tidsskrift (Health Policy journal) that we must take the cause of the increasing incidence of cancer seriously.
It's hard to disagree with that statement.
Denmark is apparently the country with the most cancer cases per capita in Europe.
This is shocking news! No data is provided to support the claim, but Jesper Fisker is undoubtedly right.
There is hardly anyone who would oppose the good intentions of taking prevention and early diagnosis seriously. Of course, we must focus on where we can actually make a difference.
The question is where should we start?
Prevention and early diagnosis must necessarily be linked to reliable data on “why”.
Even though fewer people are smoking, the incidence of cancer is apparently increasing.
It's mysterious.
According to Jesper Fisker, a significant part of the explanation for the high cancer burden in Denmark is smoking. “Every year, around 16,000 people die from tobacco-related diseases.” This claim is not documented with solid data or evidence.
It's probably a good idea not to light the first cigarette. Agreed.
Excess mortality.
Let's start with the data and the assumptions.
Jesper Fisker writes that more people will get cancer as the population ages.
I would like to doubt that the population is actually getting older.
That curve was broken in 2021!
It has been documented in several demographic studies that excess mortality has increased not only in Denmark but throughout the world since 2021.
You cannot have an aging population and a catastrophic excess mortality rate of approximately 5-10% for Denmark in 2021 and 2022 at the same time. The two factors are incompatible. That is common sense.
Who is claiming that we are getting older?
Our health authorities are. Do they have an interest in maintaining that claim even though it doesn't align with real world data?
This could be relevant if the authorities want to cover up the real cause of the excess mortality.
Let's get some data on the table: When did excess mortality start?
It apparently started in 2021.
What happened in 2021?
A mass injection of an experimental conditionally approved product was carried out on approximately 80% of the population.
Was there a temporal correlation with excess mortality and these products?
Yes. This is a fact both In Denmark and in many other countries in the world.
Figure 1. below by M. Schmeling is based on official data for Denmark (Statbank.dk)
If we look more closely at the figure, there is a small increase in 2018, probably this small peak is an expression of the influenza epidemic in 2018.
We did not hear much about that "pandemic".
In 2020, when we had what is supposedly the largest pandemic in human history, there was no excess mortality in Denmark. Strange.
In 2021, however, when mass injections were imposed even on young people, children and pregnant women - out of consideration for others, of course - there was a sharp increase in mortality in temporal relation to these injections.

Figure 1.
Let's look at excess mortality in other parts of the world.
Since 2021, non-COVID excess mortality has been observed in many countries with high COVID-19 vaccine coverage, particularly in younger age groups (2,3,4,5,6,7). This increase was accompanied by an increase in disability claims (8) and was observed in countries such as Australia and Singapore (9, 10).
Since these countries had high vaccination coverage but a lower incidence of COVID-19 infections, it is a relevant scientific question to investigate the cause of this excess mortality.
A study by Sorli (2) reported that 6.08 million more people died in 2021 than in 2020. This contrasts with modeling studies that claimed that COVID-19 vaccination saved 14 million lives (11). A conclusion that relies on questionable assumptions (12). Sorli’s analysis of real-world data suggests that
The mortality rate in the vaccinated population in 2021 was 14.5% higher than in the unvaccinated population.
The largest study, covering 125 countries in the world, was conducted by Denis Rancourt, Joseph Hickey and Christian Linard: They find a worldwide excess mortality of approximately 30 million people in the period from 2020 to 2022 inclusive.
Of these, approximately 17 million deaths are calculated to be associated with the COVID19 vaccines (3).
They argue for probable mechanisms and conclude that there are three primary causes of death associated with the increased mortality from all causes during (and after) the Covid period. These causes are:
Biological (including psychological) stress from mandates such as lockdowns and associated socio-economic structural changes
Medical interventions unrelated to the COVID-19 vaccine, such as mechanical ventilators and medications (including refusal of antibiotic treatment)
Rollout of COVID-19 vaccine injections, including repeated rollouts on the same population groups
These researchers later looked more closely at mortality data from 2020 during the COVID19 pandemic (4).
Large spikes in overall mortality occurred immediately following the World Health Organization (WHO) declaration of the COVID-19 pandemic on March 11, 2020.
These large spikes in mortality were not due to a new and virulent virus (SARS-CoV-2) spread by human contact – the alleged first wave of infection.
The aforementioned highly qualified researchers tested the assumption of the alleged virus spread paradigm using high-resolution spatial and temporal variations in all-cause mortality in Europe and the United States.
The researchers examined all-cause excess mortality for subnational regions in the United States and Europe in March-May 2020, which we call the "first peak period", and also in June-September 2020, which we call the "summer peak period".
Data reveal several definitive features that are inconsistent with the viral spread hypothesis:
• Geographical disparity in excess mortality during the first peak period: There was a high degree of geographical heterogeneity in excess mortality in the United States and Europe, with a handful of geographic regions having largely synchronous (within a few weeks of each other) large spikes in excess mortality during the first peak period while all other regions had low or negligible excess mortality during said first peak period.
( Under normal circumstances, viruses do not stop at borders or skip states)
• Temporal coincidence of excess mortality during the first peak period: The peaks for the US states and the European countries were almost all within three or four weeks of each other and never earlier than the week in which the WHO declared the pandemic.
(As one would expect if it were a viral pandemic)
• Large differences in excess mortality in the first peak period for comparable cities with major airports in the same countries: There was a dramatic difference in excess mortality in the first peak period between the compared cities, despite having similar demographics, healthcare systems and international air traffic, including from China and East Asia.
They also examined data on the place of death (whether it was in hospital, at home, in a nursing home, etc.) and socioeconomic vulnerability (poverty, minority status, overcrowded housing, etc.) at high geographic resolution, supporting an alternative hypothesis that the excess mortality in areas with large peaks was caused by the use of dangerous medical treatments (especially invasive mechanical ventilation and pharmaceutical treatments) and pneumonia caused by biological stress resulting from treatment and lockdown measures.
Unusually large peaks occurred in areas with large publicly funded hospitals.
Overall, their study provides strong evidence that the patterns of excess mortality observed in the United States and Europe in March–May 2020 could not have been caused by a spreading respiratory virus , but instead were due to the medical and government interventions that were used, mainly killing the elderly and poor.
Cancer
Could there be other reasons for the increase in cancer than smoking?
Jesper Fisher writes:
“The Danish Cancer Society, together with a number of leading organizations, has urged Christiansborg (the Danish Government) to adopt a plan for the gradual phasing out of tobacco and nicotine - with a clear goal that tobacco and nicotine will no longer be sold as regular consumer products in Denmark after 2035. ”
So a total ban.
Let's first look at the smoking habits of the Danish population. The figure below is from cancer.dk , the Danish Cancer Society's own data.

Figure 2.
The proportion of Danes who smoke has fallen from approximately 60% to approximately 17%!
It is a huge success that fewer people smoke. A success achieved mainly through volunteerism.
And yet the incidence of cancer is increasing.
It is obvious that other significant causes for the increasing incidence of cancer must be sought.
Why should we aim for a total ban on tobacco by 2035? It seems like a diversionary tactic.
Ute Krüger, a Swedish chief physician in pathology and author of the histopathological atlas “vaccinated – dead” has many years of experience studying breast cancer tissue. In the fall of 2021, she noticed that more and more younger women were being diagnosed with fast-growing breast cancers. She called them turbo cancers. She noted that they were temporally linked to the COVID-19 vaccinations (13). She warned the Swedish Health Authorities, firmly believing that they would take the matter seroius. But no.
And she warned the world.
Since Ute Krüger warned about the increased incidence of breast cancer after the COVID19 gene therapy vaccines, a lot of research has been done on the connection between cancer and mRNA COVID19 injections.
Below is a compendium of scientific studies indicating that COVID genetic vaccines can cause cancer, hyper-progressive cancer, and cancer reactivation through 20 different, independent mechanisms that may act synergistically (14).
Here are just 3 of the 20 mechanisms described in the compendium. Vaccine spike protein, which is produced in the body's cells following the instructions from the synthetic mRNA, can induce cancer by the following mechanisms:
An increased risk of blood clots (15,16,17): Spike induces coagulation states. It is known that a person with cancer is prone to increased blood clotting ability, and this in turn contributes to the development of cancer.
Inhibition of p53 (tumor suppression): A very important protein that is produced in the body for apoptosis (cancer cell death) to occur, thus preventing cancer cells from dividing (proliferating).
Alteration of the RAA system (renin-angiotensin system) (18,19,20): This system, in addition to regulating blood pressure, is associated with certain aspects that can worsen cancer, such as metastasis.
Residual DNA in the COVID19 mRNA injections:
The presence of residual DNA in the final product, as an unavoidable part of the manufacturing process, has been found in several studies by independent researchers to be several times above the legally acceptable limit (21, 22). The presence of residual DNA, and in particular the SV40 promoter/enhancer, has raised great concern due to its genotoxic potential, as pointed out in the NORTH Group’s letter of concern to the Minister of Health and the Prime Minister in November 2024 (23) .
Although health authorities have not openly established a link, some data suggests changes in cancer incidence since 2021. Figure 3 below shows an increase in the number of young people in the UK seeking financial support due to a cancer diagnosis (24).
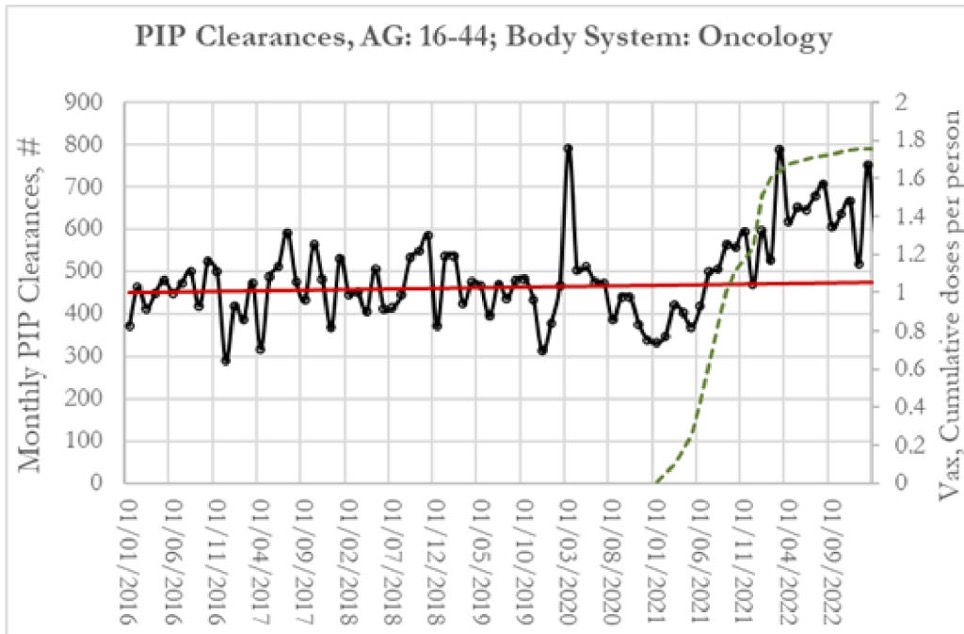
Figure 3. Personal Independence Plan (PIP) applications, January 2016-February 2023, UK.
Figure 4 below shows that spending on cancer treatment has taken a historic leap upward since 2022 in the United States (25).

Figure 4.
Two scientific studies in particular have linked COVID19 mRNA injections to cancer (26, 27):
A South Korean analysis of the national cohort of approximately 8.4 million people found increased risks of hematological and other specific malignancies after COVID19 vaccination (26)
A 30-month cohort study in an Italian province reported a significant increase in cancer hospitalization rates among the vaccinated population (27).
These signals at the population level are worrying and should be investigated and verified at the Danish national level.
These studies cannot be swept under the carpet, especially not by the Danish Cancer Society.
SV40 sequences have been found in studies of Pfizer’s Covid-19 vaccine, which were not reported by Pfizer to the regulatory authority. SV40 sequences are known to be oncogenic (cancer-causing) and to, among other things, direct DNA into the cell nucleus (28).
The Danish Medicines Agency (LMST), on behalf of the Minister of Health, has confirmed the presence of very small “fragments” of SV40 virus in Pfizer vaccines (29).
Quote:
" It is unlikely that the SV40 fragments used in Pfizer's plasmid can behave in any way like the full virus, and therefore these fragments pose no risk of developing cancer , nor can they insert/alter the human genome ."
This answer distorts the facts!
This specific small SV40 fragment – not the entire virus – is usually used in gene therapy when changes in genes are desired (30).
Are the drug authorities not aware of this?
The LMST also admitted that:
Quote
" It is correct that it was not specified in the application from Pfizer that the DNA plasmid contains small pieces of SV40 sequences. "
My next question: Shouldn't this omission in the application have consequences for Pfizer?
That question remained unanswered.
Reference is made to the NORTH group's lay summary, which describes the main concerns and mechanisms of harm associated with these mRNA products (31).
Conclusion:
If health and drug safety authorities do not act transparently and on the basis of science without conflicts of interest, healthcare professionals will not be able to provide patients with the safety information necessary for informed consent. Science is not infallible and rarely even independent, and often financial and political interests make it difficult and slow to bring errors and conflicts of interest to light.
We must be able to trust that the statistics of official authorities reflect reality and that experts are listened to, even if their observations or concerns contradict the statistics or the authorities' information.
Jesper Fisher writes
The Danish "Cancer Plan V contains important steps in the area of prevention, including an age limit for tanning bed use and fewer points of sale for tobacco and nicotine. But the decisive measures that can create lasting gains are still missing. My Christmas wish is that the upcoming Public Health Act delivers precisely those measures."
Sounds good, but are these measures the right ones?
What about ultra-processed foods, food additives, nanoparticles in medicine, clothes and cosmetics? And what about the lack of vital sunlight (UVB) and natural vitamin D? In addition, there is the well-being in families, which is unlikely to be improved by more shaming, coercion and control.
There are many important areas to look into beyond the obvious, namely the experimental Covid 19 genetic vaccines.
The fight against cancer and the Minister of Health's unilateral focus on smoking as a cause is unsustainable.
Therefore, we once again urge that not only the Danish Cancer Society, but also the regulatory authorities, national and international health and hospital authorities be aware of this.
First step: It is strongly recommended that health authorites
Stop the use of the genetic COVID19 mRNA vaccines immidiatly!
Issue a health warning to the population as well as
Develop a protocol for cancer diagnostics and implement it with the aim of making an early diagnosis to save as many lives as possible.
References:
1. Jesper Fisker. The fight against cancer. https://sundhedspolitiskistidsskrift.dk/debat/10993-danmark-har-europas-hojeste-kraeftforekomst-vi-skal-tage-hvorfor-alvorligt.html
2. Sorli S. The Discrepancy Between the Number of Saved Lives with COVID-19 Vaccination and Statistics of Our World Data. https://www.longdom.org/open-access/the-discrepancy-between-the-number-of-saved-lives-with-covid19-vaccination-and-statistics-of-our-world-data.pdf?utm_source=substack&utm_medium=email
3. Denis Rancourt et al. Spatial-temporal variation in all-cause excess mortality in the world (125 countries) during the Covid period 2020-2023. Correlation-Canada.org . https://correlation-canada.org/covid-excess-mortality-125-countries/
5. Mostert S et al. Excess mortality across countries in the Western World since the COVID-19 pandemic: 'Our World in Data' estimates of January 2020 to December 2022. https://bmjpublichealth.bmj.com/content/2/1/e000282
6. Alessandria M et al. A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province. https://www.mdpi.com/2076-2607/12/7/1343
7. Wrigley-Field E et al. Mortality Trends Among Early Adults in the United States, 1999-2023. https://pubmed.ncbi.nlm.nih.gov/39888620/
10. https://hartuk.substack.com/p/the-impact-of-synthetic-spike-protein?utm_source=publication-search
11. Watson OJ, Barnsley G, Toor J et al. Global impact of the first year of COVID-19 vaccination: a mathematical modeling study. Lancet Infect Dis . 2022;22:1293-302. doi:10.1016/S1473- 3099(22)00320-6
13. Krüger U. et al. Vaccinated - dead. www.histo-atlas.com
14. Marco Albertazzi, MBA. Dr. Karina Acevedo Whitehouse, PhD: 20 distinct, independent and possibly synergistic mechanisms of action in which genetic COVID vaccines can produce cancer, hyper-progressive cancer and/or its reactivation.
15. Villacampa A, Alfaro E, Morales C, Díaz-García E, López-Fernández C, Bartha JL, López-Sánchez F, Lorenzo Ó, Moncada S, Sánchez-Ferrer CF, García-Río F, Cubillos-Zapata C, Peiró C. SARS-CoV-2 S protein activates NLRP3 inflammasome and deregulates coagulation factors in endothelial and immune cells. Cell Communal Signal. 2024 Jan 15; 22(1):38. doi: 10.1186/s12964-023-01397-6. Erratum in: Cell Commun Signal. 2024 Jan 23; 22(1):64. doi: 10.1186/s12964-024-01491-3. PMID: 38225643; PMCID: PMC10788971.
16. Peng Q, Zhu J, Zhang Y, Jing Y. Blood hypercoagulability and thrombosis mechanisms in cancer patients - A brief review. Heliyon. 2024 Oct 1; 10(19):e38831. doi: 10.1016/j.heliyon.2024.e38831. PMID: 39435109; PMCID: PMC11492250.
17. Guglietta S, Rescigno M. Hypercoagulation and complement: Connected players in tumor development and metastases. Semin Immunol. 2016 Dec; 28(6):578-586. doi: 10.1016/j.smim.2016.10.011. Epub 2016 Nov 18. PMID: 27876232.
18. Giacomoni J, Sabatier JM. Renin-Angiotensin System Dysregulation: ADAM17 Activation Consequences Related to SARS-CoV-2. Infect Disorder Drug Targets. 2025; 25(1):e290424229522. doi: 10.2174/0118715265299597240422102455. PMID: 38685806.
19. Subbarayan K, Ulagappan K, Wickenhauser C, Bachmann M, Seliger B. Immune Interaction Map of Human SARS-CoV-2 Target Genes: Implications for Therapeutic Avenues. Front Immunol. 2021 Mar 16;12:597399. doi: 10.3389/fimmu.2021.597399. PMID: 33796097; PMCID: PMC8007772.
20. Miranda FS, Guimarães JPT, Menikdiwela KR, Mabry B, Dhakal R, Rahman RL, Moussa H, Moustaid-Moussa N. Breast cancer and the renin-angiotensin system (RAS): Therapeutic approaches and related metabolic diseases. Mol Cell Endocrinol. 2021 May 15;528:111245. doi: 10.1016/j.mce.2021.111245. Epub 2021 Mar 20. PMID: 33753205.
21. König and Kirchner: Methodological Considerations Regarding the Quantification of DNA Impurities in the COVID-19 mRNA Vaccine Comirnaty ® https://pmc.ncbi.nlm.nih.gov/articles/PMC11130870/
22. Speicher et al: Quantification of residual plasmid DNA and SV40 promoter-enhancer sequences in Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada https:// www.tandfonline.com/doi/full/10.1080/08916934.2025.2551517#abstract
25. Ethical skeptic https://theethicalskeptic.com/2025/02/17/the-state-of-things-pandemic/
26. Kim, H., Kim, MH., Choi, M. et al. 1-year risk of cancer associated with COVID-19 vaccination: a large population-based cohort study in South Korea. Biomark Res 13, 114 (2025). https://doi.org/10.1186/s40364-025-00831-w
27. Martellucci A, et al. (2025). COVID-19 vaccination, all-cause mortality and hospitalisation for cancer: 30-month cohort study in an Italian province. https://doi.org/10.17179/excli2025-8400
28. Senigl F, et al. (2024). The SV40 virus enhancer functions as a somatic hypermutation targeting element with potential tumorigenic activity. https://www.sciencedirect.com/science/article/pii/S266667902400017X

Comments